
Niacin also called as “Pellagra preventive factor / P-P factor” was coined by Goldberger in regards with its efficient role in curing pellagra. Pellagra (Italian word “pelle” means skin and “agra” as rough) in 1900s spawned skin rashes and other harmful symptoms in mental asylums and orphanages. From what is known, the epidemic called for research on what causes this prevalent condition especially among the convicts of mental asylum but not the staff. Thorough study of peculiarities between the two revealed the diet of pellagrins consisted of rice, corn, sweet potato etc. However, dried meat or liver in diet helped eradicate the symptoms.
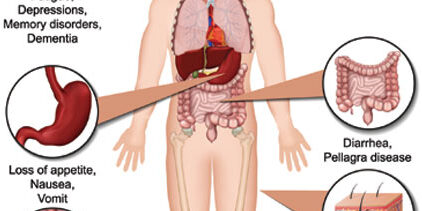
Niacin, a pyridine derivative, when taken in diet appropriately yields the coenzymes NAD+ and NADP+. Dietary nicotinamide and tryptophan also serve the same purpose. These coenzymes then perform the oxidation reduction reaction in the body which are important to life. The diverse functions to which niacin contributes include energy production, cellular metabolism, maintenance of nervous system, digestive system, skin, antioxidant role, cell signaling etc. Deficiency of vitamin B3 may lead to following symptoms of which the three Ds are the most prominent:
1. Skin Lesions:
Dry, rough, scaly skin, referred as dermatitis (the first D) with burning sensation is seen at the areas of the skin exposed to sunlight particularly the extensor surfaces of forearms. Pressure, heat or trauma to skin also causes it to become red, later brown, scaly and hyper-pigmented. Alcohol and high corn diet precipitates dermatitis. Occasionally, vesicles may also form at mucocutaneous junctions. Red swollen tongue, tender and fragile gums, angular cheilitis, hyperkeratosis and seborrhea are other reported symptoms.

2. Cerebral manifestations:
Neuropsychiatric features associated with Niacin deficiency are apathy and weakness at the initial stage but further worsen to headache, irritability, anxiety, depression and even psychoses, dementia (the second D), encephalopathy etc. Disorientation and delirium become apparent due to decline in brain function. Niacin normally protects the brain cells and provides cognitive performance by augmenting brain bioenergetics. Thus, its malabsorption from diet may also make brain cells vulnerable to amyloid toxicity progressing towards Alzheimer’s disease.
3. Gastrointestinal manifestations:
Poor appetite, nausea, vomiting, abdominal pain, gastritis, dysphagia, stomatitis, sore beefy tongue and diarrhea (the third D) are the clinical representations of niacin inadequacy. Achlorhydria is seen in some cases. The papillae of tongue atrophy and burning is felt along throat and esophageal walls. Diarrhea is usually watery but may also become bloody or mucoid occasionally. Alternation with constipation may also dispense.
4. Insomnia:
Niacin, a tryptophan derivative, has a role in the production of serotonin, a neurotransmitter that regulates sleep / wake cycle. Thus, niacin is a sleep aid that supports restful sleep among patients especially when taken at bedtime. Since niacin can be synthesized by tryptophan in the body, dietary intake is never required unless tryptophan supplies are adequate. Oral Niacin doesn’t cause drowsiness however, nicotinic acid depletion leads to sleep deprivation termed as Insomnia.

5. Miscellaneous Effects:
Behavioral changes such as aggression, restlessness, fatigue, lethargic are associated with depletion of high energy molecules such as NAD subject to diminished Niacin stores. Malnutrition may also aggravate. Paresthesia and tingling sensations are felt over the body surface. Stunted growth, weight loss and dehydration transpire due to persistent diarrhea. All these symptoms if untreated for a long time leads to the fourth D= Death as these altogether leaves a person with no mental and physical strength. Thus, leading to loss of life.

Dietary sources of Niacin:
Richest in animal liver, meat, kidney, eggs, milk etc.
Plant sources: Wheat, dried legumes, tomatoes


Recommended Daily Allowance/ Daily Intake:
16 mg/day for men, 14 mg/day for women, 6 mg/day for adolescents, 12 mg/day for preadolescents. Requirement increases during pregnancy, lactation, convalescence, high calorie intake, high corn diet and acute illness. High corn diet call for an additional supplementation of Niacin since maize protein “zein” is deficient in tryptophan necessary for B3 synthesis. 60 mg of tryptophan yields approximately 1 mg of niacin.
Pharmacological role of Niacin:
Niacin serves to treat hyperlipidemia in addition to treating vitamin deficiencies. Its role in causing vasodilation with flushing increases the blood flow to the skin. NAD+ and NADP+, the coenzyme forms of niacin, are responsible for the degradation of fats, proteins and carbohydrates and the synthesis of fatty acids and cholesterol. Niacin, by the formation of high density lipoprotein (HDL) cholesterol (the ‘good’ cholesterol) helps clear the blood of low density lipoprotein (LDL) cholesterol (the ‘bad’ cholesterol). The cholesterol lowering effect of niacin decreases the plasma cholesterol and hence reduces the risk of myocardial infarction.
This water soluble vitamin is absorbed from small intestine and converted to NAD+ through a cascade of reactions. digestive disorders, excessive use of the drug isoniazid which is used to treat tuberculosis and excess consumption of alcohol prevents niacin absorption.
2 responses to “5 signs of Niacin (Vitamin B3) deficiency in diet!”
[…] 5 signs of Niacin (Vitamin B3) deficiency in diet! […]
[…] 5 signs of Niacin (Vitamin B3) deficiency in diet! […]